





Ovarian hyperstimulation is a serious complication of IVF treatment. Ovarian hyperstimulation syndrome can be life threatening in severity as it can cause complications like venous or arterial thrombosis, including stroke, deep vein thrombosis of lower limbs leading to ischaemia, filling of water in the chest, abdomen, around the heart, shutting off kidney function and many other such complications.
What is ovarian hyperstimulation?
Ovarian hyperstimulation syndrome occurs when the ovaries are over stimulated and are increased in size due to formation of multiple follicles while giving gonadotropin injections in the process of IVF.
It is characterised by an unpleasant feeling of bloating, difficulty in breathing, passing very less urine, pain in abdomen due ovarian enlargement and filling of fluid in the cavities of body.
The pathogenesis of OHSS is increased in the vascular permeability and passage of fluid from the vessel lumen to the third space.
In susceptible patients, the use of hCG for final follicular maturation called trigger injection is the primary stimulus leading to this condition, due to the over-production of VEGF in the ovaries. This over-production of endothelial growth factor increases the permeability of vascular wall leading to loss of fluid in the third space giving rise to all these symptoms and signs.
There are two types of clinical OHSS, both associated with hCG.
- Early onset OHSS which manifests in the first eight days after taking hCG.
- Late onset OHSS which occurs nine days or more after taking hCG, and is related to hCG produced by pregnancy.
OHSS is potentially life-threatening and affects young, healthy patients. This can create a significant concern, bad health, economic burden, absence from work, bed rest our hospitalization leading to increase in cost of treatment in severe cases.
Although severe OHSS is very rare, but whenever occurs electrolyte disturbances can be fatal in young women undergoing infertility treatment.
Causes of ovarian hyperstimulation syndrome
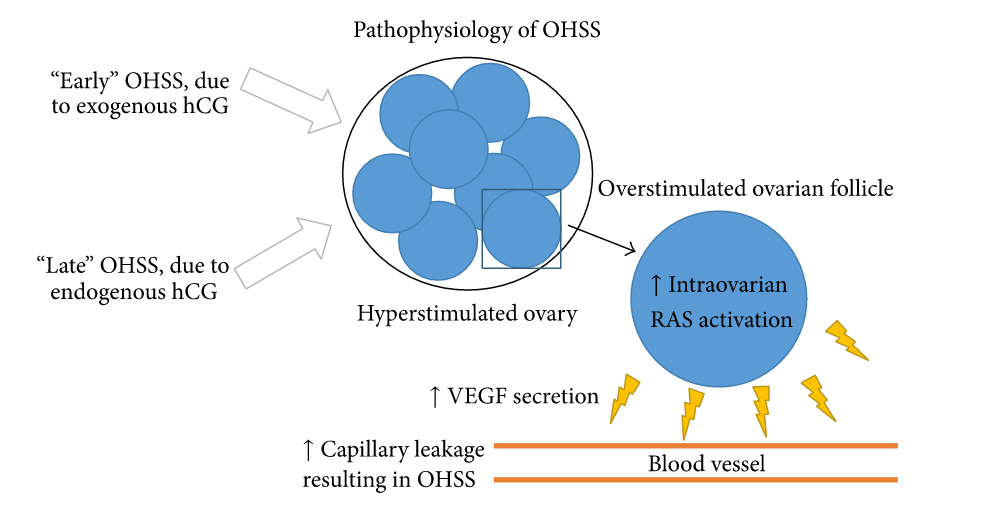
Use of gonadotropins to stimulate the ovaries with excessive of ovarian response manifested by growth of multiple follicles, high serum estradiol concentrations and an increased ovarian size. Use of exogenous hCG to trigger the final oocyte maturation causes production and release of vascular endothelial growth factors by the granulosa cells of the corpus luteum. These growth factors mainly VEGF binds with the receptors and activate the signal downstream leading to increased vascular permeability. This increased vascular permeability causes shifting of fluid from inside of blood vessels to third space causing all the symptoms.
Pregnancy after ovarian stimulation can cause increased hCG secretion from the placenta which may also stimulate increase secretion of VEGF from the ovaries and the cascade off receptor activation and increase vascular permeability follows.
who is at risk of ovarian hyperstimulation
- History of OHSS
- PCOS patient
- Biological markers like serum AMH concentrations more than 3.3 ng/ml.
- AFC more than 15.
- During stimulation number of follicles having diameter more than 10mm are more than 20 in number.
- High serum Estradiol concentrations like more than 3500pg/ml on the day of trigger.
- More the number of oocytes obtained during IVF more is the risk of OHSS.
- Use of hCG instead of progesterone for the luteal phase support.
- Pregnancy not only increases the risk of late onset OHSS but it does increases the duration and severity as well due to prolonged stimulation of ovaries by endogenous hCG.
OHSS can be classified into four stages based on the severity of symptoms, signs and test results.
Mild OHSS
Mild OHSS which is characterised by an increase in ovarian size with multiple follicles, bloating and malaise, mild nausea, vomiting but the blood tests are all normal. It is commonly seen after ovarian stimulation with gonadotropins for in vitro fertilisation. Usually no special care is needed but the patient should be monitored closely and recovery is the rule.
Moderate OHSS
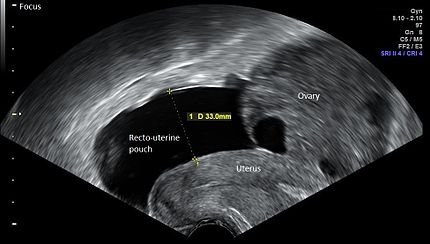
Clinical features include characteristics of Mild OHSS plus ultrasound evidence of abdominal fluid along with the increase in ovarian size up to 12 cm is there. Abdominal discomfort and gastrointestinal symptoms example nausea, vomiting and diarrhoea are frequent and more severe than mild OHSS. Blood tests will show haematocrit >41 %, WBC more than 15,000/microliter, lower Proteins.
Severe OHSS
In addition to the manifestations of moderate OHSS, severe OHSS is determined by the appearance of abdominal fluid with severe abdominal pain and some patients might have pleural effusion as well. Woman with severe OHSS can gain weight between 15 to 20 kg within 5 to 10 days and exhibit progressive leucocytosis. Ascites and pleural effusion can affect lung function leading to lack of oxygen and breathlessness.
Hypoglycaemia, decrease in urine output and increasing creatinine level > 1.6 mg/dl implies decreasing kidney function. Haematocrit >55%, WBC > 25,000/ml and electrolyte imbalance is seen. Increased blood concentration increases the risk of thrombosis.
Critical OHSS
The functions of vital organs and systems are severely compromised.
Complete cessation of urine formation, irregular heartbeat, respiratory failure, diffuse blood clots all over the body can lead to death.
Fluid around the lungs and heart can cause acute respiratory distress syndrome, top of it sepsis can complicate the clinical picture.
Diagnosis of ovarian hyperstimulation.
Diagnosis of OHSS is by clinical history and ultrasound. Factors which can predict OHSS include :
- Number of follicles during stimulation
- Maximum estradiol concentration on the day of trigger.
- Number of embryos transferred.
Once a diagnosis of OHSS is made, the severity of disease must be classified as mild, moderate, severe or critical and treated accordingly.
Prevention of OHSS
Pre treatment :
- weight management
- Insulin sensitising agents
- Recognise patients at high risk like PCOS or history of OHSS.
During stimulation :
- Tailor-made stimulation protocols
- Coasting
- GnRH antagonist cycle
- Cycle cancellation
Ovulation trigger:
- hCG dose and type
- GnRH agonist as trigger
- Recombinant LH
Ovum pick up:
- use of albumin
- Elective cryopreservation of embryos
Luteal phase support: use of progesterone
Newer techniques:
- Cabergolin
- intravenous calcium
- intravenous albumin
- Letrozole